

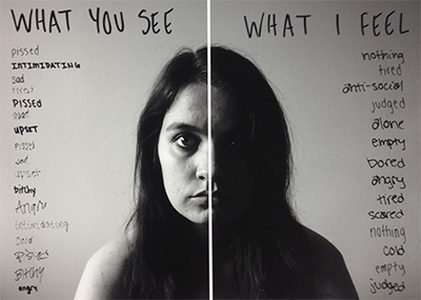
You Don't Look Depressed
/The assumption is that someone with depression is barely functional. Really, though, that is one, very far end of the spectrum of symptoms.
To further confuse things, while I am a depressive, I do not meet the clinical definition of depression when I take medication and use positive coping strategies. This is the trouble with an illness that does not have definitive blood tests, scans, or other medical identifiers. A depression diagnosis relies on a person remembering how they have felt within the last few weeks.
Self-reporting has it’s limitations, and, as a result, so does accurate diagnosis of mental illness.
The physical illness equivalent would be if my doctor diagnosed a brain tumor using only my explanations of how I perceived my symptoms. See how that could be a problem for obtaining an accurate diagnosis? What I tell the doctor might indicate the presence of a tumor, but my descriptions are hardly definitive.

“We’re all mad here.”
The invisibility of mental illness creates grey area, and grey area makes it difficult to pinpoint the cause. For much of my teenage years, figuring out why I felt so awful was like trying to find a black cat in a dark room. Sure, I eventually found it, but for much of the time I was equally concerned that there was no cat.
The Diagnostic and Statistic Manual of Mental Disorders, or the DSM-5, lists criteria for medical professionals to diagnose major depressive disorder (also known as clinical depression).
“The individual must be experiencing five or more symptoms during the same 2-week period and at least one of the symptoms should be either (1) depressed mood or (2) loss of interest or pleasure.”

Depressed mood most of the day, nearly every day.
Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day.
Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day.
A slowing down of thought and a reduction of physical movement (observable by others, not merely subjective feelings of restlessness or being slowed down).
Fatigue or loss of energy nearly every day.
Feelings of worthlessness or excessive or inappropriate guilt nearly every day.
Diminished ability to think or concentrate, or indecisiveness, nearly every day.
Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
“To receive a diagnosis of depression, these symptoms must cause the individual clinically significant distress or impairment in social, occupational, or other important areas of functioning. The symptoms must also not be a result of substance abuse or another medical condition.”
Here’s the problem, someone could have 1) depressed mood, and 5) fatigue nearly ever day, and not meet the definition of major depressive disorder! Conversely, someone could have a little bit of all of these, and not feel “significantly hampered”. In those cases, we move away from major depressive disorder, and into the realm of dysthymia, or persistent depressive disorder. Good therapists and psychiatrists can read between the lines, and know that the DSM-5, like a rulebook in a sport, is a useful guide for cataloging symptoms, and not infallible instructions from a book of holy scripture.
Feel lost yet? Don’t worry, the human brain has more connections between neurons than stars in the observable universe. Understanding the complex ways in which the mind can short-circuit is no easy task.
To aid in your understanding, below you will find one of the best lectures I have ever heard on the physiological causes of depression, and the havoc that depression wrecks on the body. Dr. Robert Sapolsky, aside from being an expert on stress, is a master of weaving scientific studies with humorous anecdotes to make for a truly lively learning experience.

