What is Project Semicolon?
/I could explain the misunderstood nature of the semicolon, but The Oatmeal does it so much better.
“Project Semicolon is an organization dedicated to the prevention of suicide. Our work is based on the foundation and belief that suicide is preventable and everyone has a role to play in preventing suicide. Through raising public awareness, educating communities, and equipping every person with the right tools, we know we can save lives.”
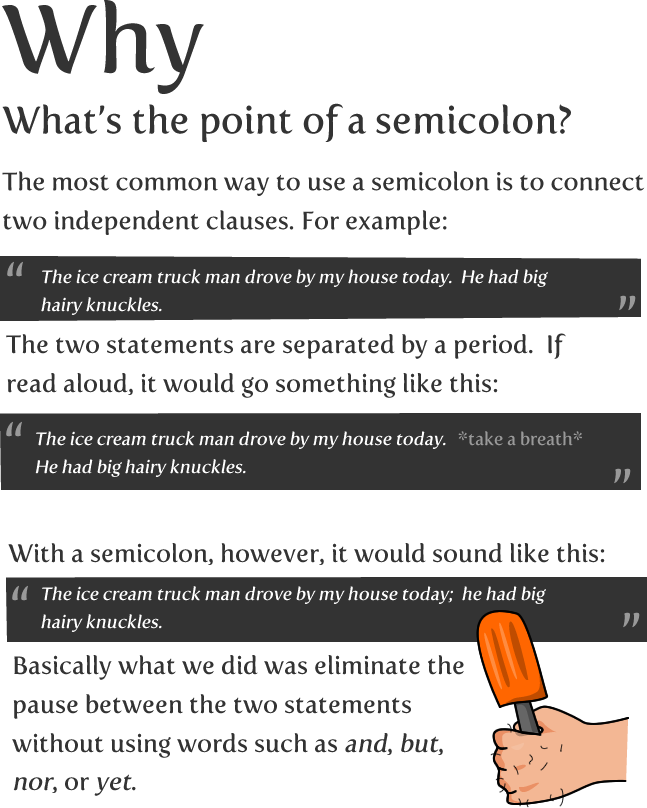
Why use a semicolon as a logo for suicide prevention? Because a semicolon is where an author could have ended a sentence; instead choosing to continue the story.
The idea is that we are all authors of our lives; those that attempt suicide metaphorically attempt to put a period at the end of theirs.
I tried to put a period on my life a couple times; I did not succeed.
A few years ago, I saw someone with a tattoo of a semicolon on their wrist. I was unsure of what it symbolized, other than an affinity for generally-misunderstood punctuation. So I went up to this person and asked… I’m kidding, I Googled it.
That search led me to Project Semicolon and to a wealth of stories that mirrored mine. As a fan of tattoos, it was not long before I walked into Read Street Tattoo and asked for one on my wrist.

Yes, that is a Llama in tree pose. My sister painted it, and it’s the best Llama painting in the world. http://caitlincorsetti.com/
You may notice that my semicolon is not oriented correctly (this makes it an Arabic semicolon). That is mainly so the sweeping tail of the punctuation covers a scar on my wrist. I earned that scar due to stupidity; putting my hand through a window in anger.
What I have come to deeply appreciate about my tattoo is that some people will ask me about it, but others will see it and say, “me too,” or “my wife.”
Or I’ll trade a subtle head nod with someone waiting in line at the grocery store.
Despite the use of a semicolon as a moderate pause in speaking; it has generated a great deal of memorable conversations.
So now you know what a semicolon tattoo means. Someone may have made an attempt. Someone may know a friend or family member who tried to die by suicide. It means the story isn’t over.
Gordon tried to die by suicide; he survives.

https://projectsemicolon.com/ - beautiful in style and placement.